Headache
Osteopathy for Headache

Types of headaches
- Vascular: migraine and cluster headaches
- Tension: muscular contraction
- Cervicogenic: referred from neck structures
- Pressure: inflammatory: tumour, infection
- Cranial neuralgia: facial pain: trigeminal neuralgia, temporal mandibular joint/muscular pain (TMJ)
- Psychotic pain: delusional explanation of pain ie “feels like worms crawling”.
- Eye strain and sinus problems can also cause headaches along with dehydration.
What headache have I got?
Diagnosis is the difficult part and I guess the main reason for not responding to treatment or medication. Cervicogenic headache pain is usually one sided referred from muscles or joints of the neck but neck pain and shoulder tension is also a common symptom of migraine sufferers. It is however thought that tension -type and cervicogenic headache suffers have more myo-fascial involvement than migraine sufferers. Headaches due to eye-strain is also a common diagnosis but if the headache occurs in the morning it is unlikely to be due to eye-strain, more likely if the headache is during or after a days work.
What an Osteopath will do?
An osteopath will ask many questions, some of which you may think irrelevant but this is necessary for both your safety as a patient and for the osteopath to decide whether it is treatable osteopathically or if further examinations are required by your GP or a specialist. You are likely to be asked, when it started, location of pain, if there is a daily pattern, what kind of pain and how severe, duration of the headache, is it seconds, hours, days, is there a trigger or does a particular movement aggravate it, do you have visual changes or any fever, sore throat or a stiff neck.

Some tests and an examination will follow the questioning, active and passive movements of the neck and spine, possibly blood pressure and a neurological examination if felt necessary. Treatment will begin once the osteopath is happy that your headache has a musculo-skeletal component and no red flags. Red flags are more worrying symptoms that may accompany the headache that would require referral to a GP, specialist or although uncommon to A&E, such as severe pain/worst ever headache or a rash and neck stiffness.
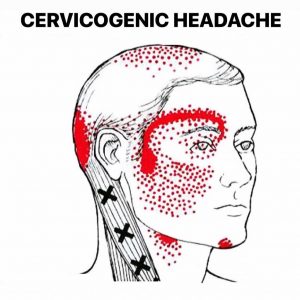
Cervicogenic headaches
This type of headache are chronic and one sided referred to the head from bony or soft tissue structures of the neck. Trigger points are hyper-irritable regions of contracted muscle which have a reduced pain threshold and refer pain in predictable patterns. Trigger points in the upper shoulders, between the shoulder blades and sub occipital muscles refer pain to the head up on finger pressure.
Osteopathic treatment
Trials have show that a combination of manual therapy, such as osteopathy alongside an exercise programme led to long-term control of these tension-type headaches. In 2004 it was shown by Bronfort that manual manipulation treatment was as effective, short term for chronic headaches, as prescribed drugs such as amitriptyline, but with much fewer side effects .

Osteopaths may use many techniques to help ease headaches, from manipulation of the neck and upper spine joints to gentle soft tissue massage ,dry needling /trigger point therapy and acupuncture. some stretching exercises may be given with advice on posture correction and possibly discuss an exercise regime.
Read more about headache here…Colgan Osteopath in Kettering Northamptonshire
Call us to see how we can help 07738493974 or book online
Cervicogenic Headache
Definition/Description
Cervicogenic headaches are chronic and one sided referred to the head from bony or soft tissue structures of the neck. It arises from the atlanto-occipital and upper cervical joints and perceived in one or more regions of the head and/or face. These occur due to a neck disorder or lesion and feature the converging of trigeminal and cervical afferents in the trigeminocervical nucleus within the upper cervical spinal cord.
Cervicogenic headaches can mimic migraines, so it may be difficult to distinguish a cervicogenic headache from a migraine headache. The primary difference is that a migraine headache is rooted in the brain, and a cervicogenic headache is rooted in the cervical spine (neck) or base of the skull region.
Some headaches are caused by eyestrain, stress, tiredness, or trauma. If you feel a headache coming on, you may be able to isolate the cause. Cervicogenic headaches are different because they are caused by problems with the nerves, bones, or muscles in your neck. Although you may feel pain in your head, it doesn’t start there. Instead, the pain you feel is referred pain from another location in your body.
The term cervicogenic headache (CGH) was coined almost 3 decades ago, and the general condition of pain located in the head but originating in the cervical spine was described over 100 years ago. It is similar to other non-specific spinal conditions in its relative lack of high level evidence regarding pathoanatomical etiology.
What are symptoms of a cervicogenic headache?
In addition to a throbbing head pain, symptoms of a cervicogenic headache may include:
- pain on one side of your head or face
- a stiff neck
- pain around the eyes
- pain while coughing or sneezing
- a headache with certain neck postures or movement
Cervicogenic headaches can also cause symptoms similar to migraine headaches, such as light sensitivity, noise sensitivity, blurry vision, and an upset stomach.
Challenging to diagnose clinically, but often includes the below:
- Unilateral “ram’s horn” or unilateral dominant headache (Excluding those with bilateral headache or symptoms that typify migrane headaches).
- Exacerbated by neck movement or posture
- Tenderness of the upper 3 cervical spine joints
- Association with neck pain or dysfunction
Pain that stays in one spot, like the back, front, or side of your head or your eye
With a cervicogenic headache, pain will often start of in the neck region first, whereas it normally starts in the head with Migraine’s and tension-type headache sufferers. Cervicogenic headaches are also side- specific and do not fluctuate from side to side like a migraine headache can.
Clinical relevant anatomy
The cervical spine consists of 7 vertebrae, C1 to C7. The cervical nerves from C1 to C8. The first two vertebrae have a unique shape and function. The upper vertebrae supports the skull, articulates superiorly with the occiput (the atlanto-occipital joint) and is named the atlas (C1).
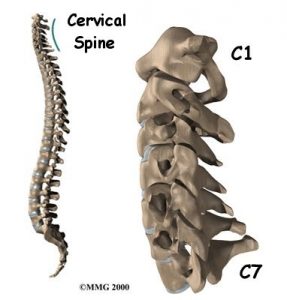
This joint is responsible for 33% of flexion and extension.The design of the atlas allows forward and backward movement of the head. Among the atlas is the axis (C2) that allows rotation. The atlantoaxial joint is responsible for 60% of all cervical rotation. Both form the upper cervical spine. The 5 cervical vertebrae that make up the lower cervical spine, C3-C7, are similar to each other but very different from C1 and C2.
Mechanism
Medical experts believe that the reason neck pain can cause a headache is due to the ‘convergence’ (the coming together) of sensory nerve fibres from the neck and sensory nerve fibres from the trigeminal nerve (the nerve that supply’s the sensation of the face and scalp). This convergence effectively makes it very difficult for the brain to interpret where exactly the pain is coming from and effectively transmits signals related to what we typically feel when we have a headache. This is why it is often called referred pain.
The mechanism which is responsible for the pain consists of a merger of the spinal nerves C1, C2 and C3, and a branch of the 5th cranial nerve, the trigeminal nerve. This merger of nerves makes it possible that upper cervical pain radiates to regions of the head which are innervated by the cervical nerve (auricular and occipital). The merger with the trigeminal afferents allows the pain to radiate to the parietal, frontal and orbital regions.
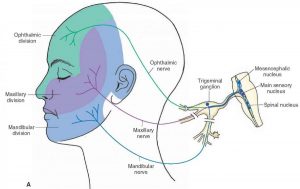
The trigeminocervical nucleus is a region of the upper cervical spinal cord where sensory nerve fibers in the descending tract of the trigeminal nerve converge with sensory fibers from the upper cervical roots. This convergence of nociceptive pathways allows for the referral of pain signals from the neck to the trigeminal sensory receptive fields of the face and head as well as activation of the trigeminovascular neuroinflammatory cascade. Also relevant to this condition is the convergence of sensorimotor fibers of the spinal accessory nerve (CN XI) and upper cervical nerve roots, which ultimately converge with the descending tract of the trigeminal nerve. These connections may be the basis for the well-recognized patterns of referred pain from the trapezius and sternocleidomastoid muscles to the face and head.
Musculo-Skeletal structures that also may contribute to headache
Sub Occipital muscles

Trigger points may occur in these muscles (see image above) which may refer pain to the back of the neck, side of the head, the eye and forehead. severe headaches can refer to the posterior eye from these trigger points according to the American college of Manual Medicine. These trigger points are thought to be brought on by stress, compromised posture ie cradling the phone or long hours at a PC, even the road bike cycling position causing hyper- extension of the neck can tighten these muscles and lead to headaches. Trigger points can also be aggravated by emotional stress, trauma or even nutritional inadequacy. Some sources including osteopath Philip Greenan believe that the vertebral arteries that pass close to the sub occipital muscles may become impinged by these hypertonic muscles and lead to reduced blood supply to the cranial structures and cause headaches, Travell & Simon’s however rebuke this.
Facet Joints
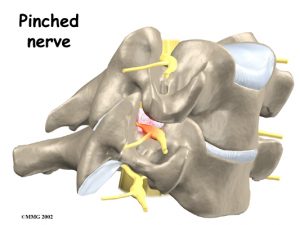
There is some evidence that multiple structures in the upper cervical spine can be the source that is referring pain into the head. The implicated structures are generally centered around C1, C2, and C3 spinal levels. This may include the joints, disc, ligaments, and musculature. The lower cervical spine may play an indirect role in pain production if dysfunctional, but there is no evidence of a direct referral pattern. Through controlled nerve blocking of various structures in the cervical spine, it appears that the zygoapophyseal joints, especially those of C2/C3, are the most common sources of CGH pain. This finding is even more common in patients with a history of whiplash.
Epidemiology/Etiology
A whiplash injury or poor sitting posture is one common cause of this type of headache. Arthritis can be a contributing factor. There are as many as 20 muscles in the neck region as well and a dysfunction in how these muscle work collectively in controlling head and neck movement can often cause significant problems.
- About 20% of those who have chronic headaches are diagnosed as having the cervicogenic type
- About 4 times as many women than men suffer from this type of headache
- The frequency and severity of a cervicogenic headache can vary greatly, but those who suffer from this type of headache often experience it on an almost daily basis.
How can Osteopathic Assessment and Treatment help?
A patient’s history and clinical presentation is vital in helping your physiotherapist to know whether their symptoms are consistent with cervicogenic headache. They will often ask you questions such as the location, severity, frequency and duration of you headache symptoms. What movements and postures typically bring on a headache episode and what you can do to make things easier.

At Colgan Osteopathy our team of highly experienced osteopaths have been trained to recognize these findings and employ appropriate manual therapy techniques to the cervical spine and associated soft tissue structures to regain range of motion and restore normal joint mechanics to the cervical spine along with instructing patients in a specific and evidence based exercise program that addresses the deep neck flexors and the stabilising muscles of the scapular area. This will also help to stimulate the process of healing and repair by facilitating normal movement and loading stresses around the symptomatic joints. Studies have documented a 76% success rate with a combination of these treatment interventions, whereby patients reported a more than 50% decrease in headache frequency and 35% achieved complete resolution of symptoms following seven weeks of treatment.
Medication for Cervicogenic Headache:
Medication alone seldom serves as an adequate treatment for cervicogenic headache although medication can sometimes provide a measure of relief. When medication is prescribed, it typically is an antidepressant, and anti-inflammatory, an analgesic, or an antiepileptic drug.
Medication-Induced Headaches:
Medication-induced headaches are more common that you may think and are caused by taking painkillers for migraines or headaches too regularly. In fact it is now recognized as the third most common cause of headache. By taking medication such as codeine, ibuprofen, paracetemol and Triptans (more specifically used for migraines) too frequently, your body becomes used to the effects of the drugs. A “rebound” or withdrawal headache may then develop if you do not take another one. As a result, you may end up getting stuck in a vicious cycle of having to rely on taking medication every day in order to keep the headache at bay.
Other types of Headaches
Acute Single Episode
Meningitis – fever, photophobia, stiff neck, rash, coma. At risk – very young. Med emergency
Encephalitis – fever, odd behaviour, fits or redused consciouness, stiff neck. At risk very young and very old, immune compromised. Med emergency
Subarachnoid haemorrhage – sudden headache +/- stiff neck. Med emergency
Tropical illness – e g malaria. +ve travel Hx, flu-like illness
Sinusitis – tender face, cold, post nasal drip. Dull constant ache over affected maxillary sinus or frontal sinus. ethmoid and sphenoid sinus P felt deep in midline at the root of the nose
Head injury – cuts/bruises, reduced consciousness, lucid intervals, amnesia. P at side of trauma or generalised. Head sinister signs suggesting subdural or extra dural haemorrhage ie drowsiness and focal signs
Cervical Artery Dissection – severe P up cervical complex. Recent Hx of mild or major trauma involving extension and/or rotation may have neurological signs 2Ns and 3Ds
Intoxication – Agg by shaking the head. Viral and other infection, alcohol, enviromental
Acute Recurrent Attacks
Migraine – pre-attack aura? visual aura? vomiting? sensitivity to light, movement, noise? recognised triggers?
Cluster Headache – typically night P in 1 eye for up to 8 weeks then OK for next few months then intermittenly repeated. Gaps may be up to 2 years. Thought to be neuralgia suspected hypothalamus involvment. Onset any age but younger men 20 plus 5;1. Pain occuresonce or twice a day;each episode lasting 15 to 160 mins. Each cluster 4 to 12 weeks. Rapid onset. Pain around one eye unilateral and mostly same side ,which may become watery and bloodshot. Pupil constriction ,eyelid drop, lacrimation, nasal discharge.
Acute Glaucoma – red eye, sees haloes, fixed big oval pupil, reduced acuity in affected eye. Nausea and vomiting. Red congested eye, cloudy cornea, non responsive pupil. Attacks may be precipitated by sitting in the dark. Mostly elderly. Constant aching P around one eye and radiates to forehead
Subacute Onset
Giant Cell Arteritis – Hx of PMR? tender scalp, >50 y o, reduced acuity (late stage). ESR elevated. Tender, thickened, pulseless temporal arteries. Ask about jaw P when eating
Chronic Headache
Tension Headache – tight band around head, non pulsative. Tension at work/home. low mood. improved by sleep
Cronically elevated ICP ( intracranial pressure) – worse on waking, focal signs. high BP, low HR. headache present in 50% of cases. Headache will wake ptn or they will wake with it. Not a severe headache, worsened by lying down. Other signs vomiting, papilloedema, epilepsy, progressive focal neurology, mental change
Medication misuse – from analgetic overuse. Mixed analgetic containing codein or prescribed opiates and triptans, causing episodic headaches to become daily headache.
Headache – Differential Diagnosis
Common causes
- Minor viral infections
- Tension type headache
- Migraine
- Acute sinusitis
- Referred neck pain
- Analgesia induced headache
- Caffeine withdrawal
- Trigeminal Neuralgia
- TMJ syndrome
- Cluster headache
- Post-concussion headache
Must Not Miss
Easily missed
Red flags
- Severe thunderclap headache
- Neurological symptoms
- (confusion, persistent focal neurological signs)
- Severe progressive headache
- New onset headache > 50 years of age
- Recent change in normal headaches
- Associated symptoms
- Petechial rash/neck stiffness
- Awoken by headaches
- Early morning headaches
- Worsened by valsalva manoeuvres
- Jaw claudication
- Temporal scalp tenderness
- Systemic symptoms (fever, weight loss)
- HIV infection
- History of cancer
Investigations to consider
- FBC, CRP/ ESR
- U&Es
- Blood & viral cultures
- X-ray (C spine, Skull)
- Lumbar puncture
- CT/MRI
- Temporal artery biopsy
- Intraocular pressure measurements
Colgan Osteopathy in Kettering @Next Step Podiatry
Address: 6 Lower Street, Kettering, Northamptonshire, NN16 8DH Press here for map
Call us to see how we can help 07738493974 or book online